This article may be too technical for most readers to understand. Please help improve ittomake it understandable to non-experts, without removing the technical details. (August 2016) (Learn how and when to remove this message)
|
Anaccessory auricle is a congenital anomaly typically seen as a skin coloured nodule, most frequently just to the front of the ear.[1][2]
| Accessory auricle | |
|---|---|
 | |
| Specialty | Dermatology |

The general presentation is of a skin-covered nodule, papule, or nodule of the skin surface, usually immediately anterior to the auricle.[2] However, it may be anywhere within the periauricular tissues.[2] Bilateral presentation can be seen.[2]
A study of a family with 11 affected showed the accessory auricle were inherited in an autosomal dominant manner.[3]
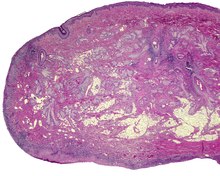
The lesions presents as a nodule or papule, either sessile or pedunculated. They may be soft or have a cartilaginous structure. By histologic examination, it is a recapitulation of normal external auricle. There will be skin, cartilaginous structures, and cartilage (although the later is not seen in all variants of this disorder).[4][5] Some investigators believe that the tragus is the only hillock which is derived from the first branchial arch. This is clearly suggestive that true cases of Accessory Auricle represent a true duplication of the hillocks that were part of the second branchial arch.[6] The second ear appears as a mirror image folded forward and lying on the posterior cheek.[citation needed]
These structures are distinctly different from squamous papilloma and benign teratoma.[citation needed]
The several components or degrees of development range from an ear tag, preauricular appendage, preauricular tag, or accessory tragus, to supernumerary ears or polyotia.[7] It is a relatively common congenital anomaly of the first branchial arch or second branchial arches. Other anomalies may be present concurrently, including cleft palate, cleft lip, or mandibular hypoplasia. There is a known association with Goldenhar syndrome (oculo-auriculo-vertebral syndrome)[8] and with Wildervanck syndrome.[9][10][11] There may also be an association with congenital cartilaginous rest of the neck.[citation needed]
Simple surgical excision is curative.[12] The recommended treatment is that the skin is peeled off the extra-auricular tissue and protruding cartilage remnants are trimmed.[13] Normal appearance is achieved in majority of cases. The reconstruction successful in true cases of accessory auricle, as it also is in individuals with auricular appendages.[14][15]
These lesions usually present in neonates, although they may not come to clinical attention until adulthood (for cosmetic reasons). There is no gender predilection. They are present in approximately 3-6 per 1000 live births.[16]